

서론
스타틴은 금세기 들어 가장 각광받는 약 중 하나이다. 개발된 지 수십 년이 지났지만 작년에만 전 세계에서 20조 원에 달하는 매출을 올렸다. 비결은 무엇일까? 수많은 대규모 임상연구를 통해 허혈성 심장질환이나 뇌졸중을 예방하는 것이 증명되었기 때문이다[1,2]. 그런 스타틴에 비견되는 당뇨병 약제가 등장했다[3]. SGLT2억제제(sodium glucose cotransporter 2 inhibitor)라 불리는 이 약은 처음 등장했을 때만 해도, 혈당강하효과는 크지 않아도 체중감소와 혈압 관리에서 두루 이점이 있는 다면효과가 있는 약제 정도로 인정되었다. 그러다가 최근 들어 심혈관질환, 심부전, 신장질환을 예방하거나 치료할 수 있는 놀라운 연구 결과들이 잇달아 발표되었다[4-14]. 그래서 이제는 당뇨병 약에서 심장약, 신장약으로 그 지평을 넓혀가고 있다. 심지어 당뇨병이 없더라도 심장이나 신장이 나쁘다면 처방해야 하는 약이 된 것이다[15,16].
본 고에서는 불과 10년 만에 ‘21세기의 스타틴’이라 불릴 정도로 막강한 약제로 등장한 SGLT2억제제의 시작부터 현재까지의 여정을 살펴보려고 한다. 이를 통해 최근까지의 연구 결과에 근거한 이 약제의 장ㆍ단점을 소개한 후, 아직 해결되지 않은 이슈와 연구 결과를 적용할 때 주의할 점을 언급할 것이다.
SGLT2억제제 연구의 역사: 넓혀지는 지평
SGLT2억제제의 원조물질이라고 할 수 있는 사과나무 껍질에서 유래된 phlorizin은 Laurent-Guillaume de Kon-inck과 Jean Servais Stas가 1835년에 처음으로 발견하였다[17]. 이후 1886년도에 Freiherr von Mering에 의해 이 물질의 당뇨(glycosuria) 효과가 개에서 증명되어 “phlo-rizin-diabetes”라는 용어가 사용되기 시작했다[17]. 이후 Na+/glucose cotransporter로 문헌에 등장하기 시작한 것은 1989년도이며[18], 실제 SGLT2억제제가 당뇨병 치료제로 등장한 것은 1990년대 후반 일본의 연구진들에 의해서이다 [19,20].
SGLT2억제제를 활용한 첫 기념비적 연구는 엠파글리플로진(empagliflozin)을 이용한 Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mel-litus Patients-Removing Excess Glucose (EMPA-REG OUTCOME) 연구로, 2015년 발표 이후 무려 8,000건에 달하는 인용을 기록했다[4]. SGLT2억제제 사용으로 심혈관사망률을 38%, 전체 사망률을 32% 감소시키는 놀라운 결과를 발표했는데 이는 심혈관질환 예방의 가장 강력한 약제로 알려진 스타틴 연구에서도 보기 힘든 결과였다. 다만 죽상경화성 병변과 직접 관련된 비치명적 심근경색증과 비치명적 뇌졸중은 줄이지 못했다. 특이하게도 EMPA-REG OUTCOME 연구에서 심혈관 사망의 이점은 연구 초기 6개월 이내부터 나타나기 시작한다. 따라서 EMPA-REG OUTCOME 연구 결과는 죽상경화와 관련되어 있는 여러 위험인자의 동시 개선, 즉 혈당, 혈압, 비만의 호전 이외의 다른 기전이 작용하였을 것으로 추정된다. SGLT2억제제는 신장보호효과도 입증하였는데, DAPA-CKD (Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease) 연구에서 다파글리플로진(dapagliflozin)은 추정사구체여과율의 50% 이상 감소, 말기신장질환의 발생, 또는 신장질환으로 인한 사망을 44% 감소시켰다[12]. SGLT2억제제의 종류와 상관없이 심부전과 신장질환의 예방효과는 일관되게 확인되었고[5-7,13], 심지어 당뇨병이 없는 대상에서도 그 효과가 증명되었다[9,10,12-14]. 당뇨병 약제로 개발되었으나, 여러 기념비적인 연구를 통해 이제는 비당뇨인의 심장과 신장을 보호하는 약제로 그 지평이 확대된 것이다[15,16].
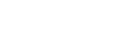
이 약제의 기본적인 이익은 나트륨배설증가(natriuresis)와 삼투이뇨(osmotic diuresis)에 의한 preload 및 after-load의 동시 감소로부터 초래되지만 이 외에도 많은 연구들을 통해 다양한 기전들이 제시되고 있다[21-25]. SGLT2억제제에 의해 증가된 케톤체가 심장기능이 떨어진 환자의 효율적인 에너지원으로 작용하여[22,23], 혹은 hemo-concentration에 따른 산소운반능력 증가가 심장보호효과를 나타냈다는 가설[24], 일종의 금식과 같은 효과(starvation mimicry)와 대사적 재프로그래밍(metabolic reprograming)이 절식의 생명연장효과와 유사한 유익을 초래하였을 가능성[25] 등도 설득력 있게 제시되고 있다. 이렇듯 SGLT2억제제는 임상에서 확인된 놀라운 결과를 이후 기전 연구를 통해 설명하려고 하는 ‘bedside to bench’ 방식의 역방향 중개연구의 대표적인 예로도 등장하였다. Fig. 1은 스타틴과 SGLT2억제제의 대규모 임상시험 결과를 비교 요약한 것이다.
Fig. 1.
Comparison of large-scale clinical trials of statins and SGLT2 inhibitors. Statins have proven cardiovascular benefits, including the primary and secondary prevention of MACE. SGLT2 inhibitors have demonstrated efficacy not only in preventing MACE but also in primary and secondary prevention of hospitalization for heart failure, even in environments where statins and RAS inhibitors are commonly used. Moreover, they have proven efficacy in reducing cardiovascular mortality and demonstrated a renal protective effect.
SGLT2, sodium glucose cotransporter 2; MACE, major adverse cardiovascular event; RAS, renin-angiotensin system; RASi, renin-angiotensin system inhibitor; ASCVD, atherosclerotic cardiovascular disease; SGLT2i, sodium-glucose cotransporter 2 inhibitor; HHF, hospitalization for heart failure; CVD, cardiovascular disease; CV, cardiovascular; CKD, chronic kidney disease.
SGLT2억제제가 필요한 대상과 부작용 이슈
SGLT2억제제와 관련된 잘 알려진 부작용은 생식기계 감염이다[26]. 여러 연구들을 통해 밝혀진 NNH (number needed to harm)는 연간 20명 정도로, 20명에게 처방할 때 한 명의 추가적인 위험이 발생할 수 있다[27]. 개인의 위생 상태가 감염의 발생에 중요한데 우리나라나 일본에서의 발생빈도는 상대적으로 낮은 것으로 알려져 있다. SGLT2억제제 등장 초기에는 이 약제의 기전상 삼투이뇨를 통해 경도의 탈수를 일으킬 수 있고 이로 인해 신기능에 나쁠 영향을 줄 가능성이 제기되었다. 그러나 SGLT2억제제는 장기적인 신장보호효과에 더해 급성신장손상의 위험성도 줄이는 것으로 보고되고 있다[28]. 따라서 신장질환이 있는 경우 꼭 처방해야 하는 약제이나, 저체중이나 영양이 결핍된 환자, 허약한 노인 등에서는 탈수나 기립성 저혈압으로 인한 위험을 고려해야 한다[29]. 하지절단이라는 안정성 이슈도 CANVAS Program (Canagliflozin Cardiovascular Assessment Study Program) 연구를 통해 제기되었으나[30], 이후 이어진 다른 약제의 대규모 연구에서는 재현되지 않았다. 다만 하지의 혈류가 좋지 않은 경우, 약제 사용 후 체액량 감소에 따른 혈액 내 점성도의 증가가 혈액순환을 더욱 악화시키고 이로 인해 말초혈관의 혈전이나 폐쇄를 초래할 이론적 가능성이 있으므로 주의는 필요하다.
당뇨병케토산증의 경우 매우 드물긴 하지만 발생 가능하다. 미국 청구자료 분석 결과를 보면, SGLT2억제제 사용 후 당뇨병케토산증으로 입원한 환자의 발생빈도는 180일 추적 결과 DPP-4억제제(dipeptidyl peptidase-4 inhibitor) 대비 2.2배(4.9 vs. 2.2/1,000 person-years; 위험비 2.2, 95% 신뢰구간 1.4 to 3.6) 높은 것으로 나타났다[31]. 절대적인 발생빈도가 높지는 않지만 SGLT2억제제 투약 후 환자가 메스꺼움과 구토, 복통, 전신무력감이나 호흡곤란 등을 호소할 경우, 특히 환자가 열량섭취를 줄였거나 과음한 경우, 췌장 기능이 나쁘거나 인슐린용량을 줄인 경우라면 케토산증의 가능성을 고려하고 감별 진단할 필요가 있다. SGLT2억제제의 부작용을 고려한 적절한 처방 대상을 요약하면 Fig. 2와 같다.
Fig. 2.
Determining Appropriate Candidates for SGLT2 inhibitor therapy. SGLT2 inhibitors should be considered for patients with heart failure or CKD and could also be a great option for those who need weight loss (blue box). However, cautious use is needed, especially for patients who have experienced frequent or consistent genital infections or those with frailty (red box). Those marked with a question mark (?) represent populations that are still under investigation or require further study to establish a concrete conclusion. Additionally, other antidiabetic agents could be considered for further intensification of glycemic control (gray box).
SGLT2, sodium glucose cotransporter 2; CKD, chronic kidney disease; SGLT2i, sodium-glucose cotransporter 2 inhibitor; eGFR, estimated glomerular filtration rate; ESKD, end-stage kidney disease; MI, myocardial infarction; NAFLD, non-alcoholic fatty liver disease; BMI, body mass index; T1DM, type 1 diabetes mellitus; LADA, latent autoimmune diabetes in adults; KT, kidney transplantation; DPP-4i, dipeptidyl peptidase-4 inhibitor; TZD, thiazolidinedione; SU, sulfonylurea; GLP-1RA, glucagon-like peptide-1 receptor agonist.
a3P symptoms: polyuria, polydipsia, polyphagia.

해결되지 않은 이슈와 연구 결과 해석의 주의점
SGLT2억제제가 엄청난 연구 결과들을 가지고 임상 현장에서 각광받고 있지만 아직 해결되지 않은 여러 이슈들이 있다. 일차예방 목적으로 메트포민 대신 우선적으로 사용해야 하나? 심근경색증 이후 재발을 예방하는 효과가 있을까? 뇌졸중 환자에서 싸이아졸리딘다이온(thiazolidinedione)이나 GLP-1수용체작용제(glucagon-like peptide-1 recep-tor agonist)에 비견할 효과를 보일 수 있을까? 말기신장질환 환자나 신장이식을 받은 환자에서도 사용 가능할까? 지방간염 환자에서 조직학적 호전을 일으킬 수 있을까? 인지능력 감소나 치매 예방에도 효과가 있을까? 1형당뇨병 환자나 당뇨병발 환자, 골절 위험이 높은 환자에서 안전하게 쓸 수 있을까? 이와 관련된 연구들이 발표되면 이후 보다 분명한 답을 제시할 수 있을 것이다.
SGLT2억제제 임상시험 결과를 해석하고 적용할 때 이 연구가 내가 임상에서 만나는 환자에게 적용 가능할지를 판단해야 한다. 심혈관질환을 이미 가지고 있는 당뇨병환자만을 대상으로 진행한 EMPA-REG OUTCOME 연구를 실제 현장에 적용하면 약 15% 환자에서만 비슷한 대상인 것으로 보고되었다[32]. DECLARE-TIMI 58 (Dapagliflozin Effect on Cardiovascular Events-Thrombolysis in Myocardi-al Infarction 58) 연구 또한 EMPA-REG OUTCOME 연구보다 연구대상자가 훨씬 더 확장되긴 했지만 이 역시 심혈관위험인자를 가진 환자들을 대상으로 했고, 참가자들의 평균 나이가 64세였다[5]. 이렇듯 임상시험 결과가 실제 내가 진료하는 환자에 적용 가능할지를 판단하려면 연구의 inclusion 및 exclusion criteria를 봐야 한다. 이것이 연구의 실제 ‘가치’에 대한 평가인데, 수많은 근거들 중 그것이 정말 내가 진료하는 환자에게 적절한지, 가치가 있는지를 평가해야 한다.
결론
특정 당뇨병 치료제가 모든 환자에게 특효약은 아니다. SGLT2억제제가 생명을 살리는 약제로 등장했지만 부작용과 주의사항도 있다. 따라서 개별 환자에 어울리는 좋은 약이 있을 뿐이다. 현재 사용 중인 당뇨병 약제는 어떤 당뇨병환자에게는 도움이 된다는 근거가 있기 때문에 승인된 것이고, 누군가에게 실제적인 도움이 될지를 판단하는 것은 ‘예술(art)’의 영역이다. 따라서 투약을 선택하고 처방할 때 당뇨병전문의는 단순히 과학자가 아닌 예술가가 되어야 한다. 환자의 혈당조절이 어려운 것이 좋은 약을 쓰지 않아서, 약을 복용하지 않아서 만이 아닐 수 있다. SDOH (social determinants of health)와 당뇨병환자의 생활습관에 나쁜 영향을 주는 요인이 있는지도 살펴야 한다[33]. 당뇨병과 관련이 없어 보이는 개인적 사건들이 실은 혈당에 영향을 줄 수도 있기 때문에 병력 청취(history taking)뿐만 아니라 ‘story taking’도 하며 환자에게 어울리는 좋은 약이 무엇인지 판단해야 한다. SGLT2억제제를 처방할 때도 환자들에게 충분한 정보를 주고 어떤 약이 적절할지 함께 공유해 공동으로 결정해야 한다. 그것이 여러 권고안에서 이야기하고 있는 공유의사결정(shared decision making)이다.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




